Here’s something most people don’t realize until they’re sitting in a pulmonologist’s office: not every COPD patient needs oxygen all day. Some need it constantly. Others only during specific activities. And understanding the difference? That’s where things get complicated.
The Numbers That Matter
Doctors make oxygen decisions based on two main measurements. First, there’s PaO2 (partial arterial oxygen tension), which requires a blood draw from your wrist. Second, SpO2 (oxygen saturation), measured with that little clip device on your finger. The clip is easier. The blood test is more accurate.
According to guidelines from the American Thoracic Society, you’re in “severe hypoxemia” territory when your PaO2 drops to 55 mm Hg or below, or when your SpO2 hits 88% or lower. That’s typically when doctors start talking about long-term oxygen therapy.
But there’s a second threshold too. If your PaO2 sits between 56-59 mm Hg (or SpO2 at 89%), and you have signs like swollen ankles, high red blood cell count, or heart rhythm changes… you might still qualify.
Think of it like this: your body’s been working overtime to compensate for low oxygen. When it starts showing strain (the heart enlarges, blood thickens, fluids build up), that’s your system waving a red flag.
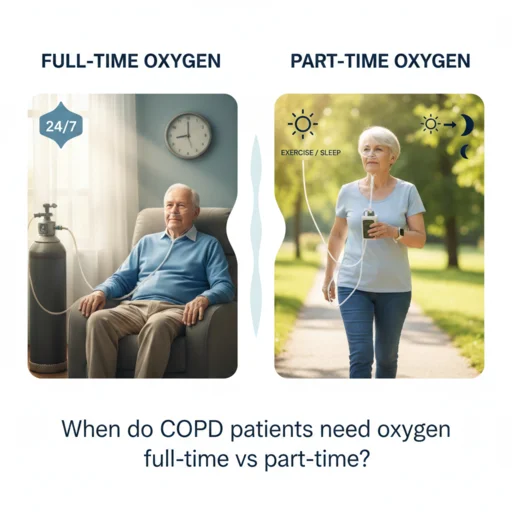
Full-Time Oxygen: The 15-Hour Rule
Here’s where the research gets specific. If you qualify for long-term oxygen therapy, you need to use it for at least 15 hours every single day. Not 10 hours. Not whenever you remember. Fifteen minimum.
This comes from two landmark studies (the NOTT and MRC trials) that showed oxygen therapy significantly improved survival in severely hypoxemic COPD patients, but only when used consistently. The patients who used oxygen 15+ hours daily lived longer than those who used it less frequently.
Most doctors recommend using your oxygen concentrator during all waking hours, plus while sleeping. That easily gets you past the 15-hour threshold and gives your body the continuous support it needs.
Why 15 hours? Because your organs (particularly your heart and brain) need sustained oxygen levels to function properly and avoid long-term damage. Sporadic use doesn’t provide the same protection.
Part-Time Oxygen: When Activities Change Everything
Now let’s talk about the other group. Some people have acceptable oxygen levels while sitting still, but drop into dangerous territory during physical activity. This is called exertional hypoxemia.
Your oxygen might read 90% while watching television. But walk to the bathroom? Suddenly, you’re at 85%. That drop matters.
The clinical threshold for ambulatory oxygen is when your SpO2 falls to 88% or below during movement or exercise. At that point, portable oxygen during activities can help you maintain stamina, reduce breathlessness, and stay active longer.
Some patients also experience nocturnal desaturation (oxygen drops during sleep) without qualifying for full-time therapy. If your levels dip below 88% for five minutes or more while sleeping, your doctor might prescribe nighttime-only oxygen. Many patients need to increase their flow rate by 1 liter per minute during sleep compared to daytime use.
The Equipment Question
Full-time users typically rely on home oxygen concentrators for most of their hours, switching to portable systems when leaving the house. Concentrators pull nitrogen from room air and deliver oxygen-enriched air through nasal cannulas. They’re economical, don’t need refilling, and can run continuously.
Part-time users often work with smaller, lighter portable concentrators or oxygen cylinders that they can take during walks, errands, or exercise. The key is matching the equipment to your specific pattern of need.
If you’re in Dhaka and need reliable oxygen equipment with quick delivery, that’s where providers like Marium Oxygen come in. They offer both sales and rentals, with 60-minute delivery inside Dhaka city and installation support included.
Target Oxygen Levels: Not Too High, Not Too Low
Here’s something that surprises people: more oxygen isn’t always better with COPD.
For most COPD patients, the target range is 88-92% saturation. Going higher than 92% can actually increase mortality risk. One study found that patients with saturations above 92% had nearly twice the death rate compared to those in the 88-92% range.
Why? COPD changes how your body handles oxygen and carbon dioxide. Too much supplemental oxygen can suppress your breathing drive or worsen carbon dioxide retention, leading to respiratory acidosis. This is particularly true for patients who already retain CO2.
Your doctor will prescribe a specific flow rate (usually 1-3 liters per minute through a nasal cannula) designed to keep you in that sweet spot. Don’t adjust it on your own.
When Oxygen Needs Change
COPD is progressive, which means your oxygen requirements can shift over time. Someone who starts with exercise-only oxygen might eventually need it full-time. Conversely, patients who start oxygen during a severe flare-up might improve enough to stop once they’ve stabilized.
That’s why follow-up testing is crucial. Medicare and most insurance providers require reassessment 60-90 days after starting oxygen therapy. Studies show that about half of patients who start oxygen during hospitalization will no longer meet criteria once they’ve recovered from the acute episode.
Your doctor should also review your prescription every six months to ensure the flow rate and usage schedule still match your needs. Disease progression, new medications, or lifestyle changes can all affect your oxygen requirements.
The Insurance Coverage Reality
Most insurance plans, including Medicare, cover oxygen therapy when medical criteria are met. That means documented hypoxemia (low oxygen levels) through either blood gas testing or pulse oximetry readings taken while you’re stable and breathing room air.
Coverage typically includes your home concentrator, portable system, tubing, nasal cannulas, and regular equipment maintenance. In Bangladesh, having a government-approved oxygen supplier like Marium Oxygen can streamline this process and ensure you’re getting properly certified medical equipment.
Living with Oxygen Therapy
Starting oxygen therapy feels like a major shift. And it is. But patients consistently report that the benefits outweigh the adjustment period.
Reduced breathlessness means you can do more. Better sleep quality because you’re not constantly gasping for air at night. Less strain on your heart. For many people, oxygen therapy is what allows them to maintain independence and quality of life despite advancing lung disease.
Safety matters too. Keep oxygen away from open flames or heat sources. Don’t smoke while using oxygen. Make sure tubing isn’t creating trip hazards. Have backup equipment for power outages (portable tanks or battery backups for concentrators).
Most importantly, use your oxygen as prescribed. Skipping sessions or cutting hours short because you “feel fine” undermines the therapy’s effectiveness. Remember, oxygen protects your organs even when you don’t feel obviously short of breath.
What to Do If You Need Oxygen
If you’re experiencing persistent breathlessness, morning headaches, confusion, or swelling in your ankles, talk to your doctor about getting your oxygen levels checked. Don’t wait until you’re in crisis.
Testing is straightforward. Your doctor will measure your oxygen saturation at rest, during activity, and possibly during sleep. If you meet the criteria for supplemental oxygen, they’ll write a prescription specifying your flow rate and when to use it.
From there, you’ll work with a medical equipment supplier to set up your system. In Dhaka, Marium Oxygen offers 24/7 customer support and can help with installation, training, and ongoing maintenance of your equipment. They handle both oxygen cylinder refills and concentrator servicing.
The bottom line? Oxygen therapy timing depends on your individual oxygen levels in different situations. Severe resting hypoxemia means full-time therapy. Drops only during activity or sleep mean part-time use. Your numbers guide the prescription, and consistency is what makes it work.